

Breast Surgery
A woman’s breasts can define her feminity.
Please scroll through the images of breasts below to try and find those which most closely resemble yours. You can then follow the link to the suggested procedure for that type of breast. Also, please vote for they type of breasts you have. It is anonymous and the information I receive is of interest to me.
The larger breasts are lower down on the page. Nipple areolar problems, Poland’s syndrome and Tuberous breasts are not well depicted, nor are breasts which have had previous surgery.
Many women have breasts like those depicted and are perfectly happy with them. I am not suggesting that everyone with that type of breast should have surgery. Presumably you have found your way to this page because you are interested in cosmetic surgery of your breasts and you are looking at this page because you are interested in some form of improvement. This page is aimed at women with that in mind.
The procedures are suggested as a guide and are no alternative to a consultation. The image is above and the describing text beneath the image in every case.

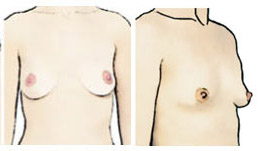
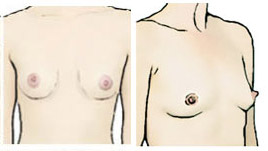
1. The ideal, although patients with this kind of breast may still want to go bigger. Breast augmentation. (5%)

2. Hypoplastic. Breast augmentation. (3%)

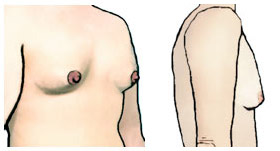
3. Hypoplastic. Breast augmentation. (4%)
4. Hypoplastic and empty. Breast augmentation. (2%)
5. Hypoplastic and empty. Breast augmentation. (5%)
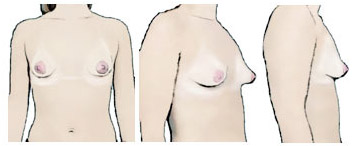
5. Tuberous type. The pictures shows the constricted base of tuberous breasts, but frequently patients also have an enlarged areola due to herniation of the beast tissue into the areola. Commonly asymmetrical with one side worse than the other. Breast augmentation may suffice although patients may need some kind of unfurling procedure too.
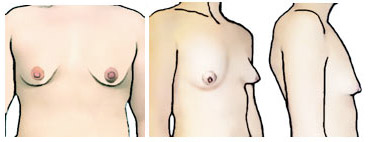
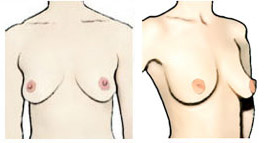
6. Tuberous type. The pictures shows the constricted base of tuberous breasts, but frequently patients also have an enlarged areola due to herniation of the beast tissue into the areola. Commonly asymmetrical with one side worse than the other. Breast augmentation may suffice although patients may need some kind of unfurling procedure too. (2%)

7. Empty or deflated. Commonly after breast feeding. Breast augmentation. (1%)

8. Full upper pole. Rarely a primary issue, usually occurring after breast augmentation with a high riding implant. If an implant is place, then this needs adjusting and correcting. Otherwise the treatment would be breast augmentation. (1%)

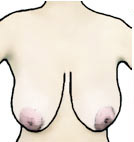
9. Empty or deflated. Commonly after breast feeding. Breast augmentation. The fullness in the armpit is an accessory breast (also called an axillary breast) and if small can be treated with liposuction. If large then it is cut out but this leaves an overlying scar. (2%)
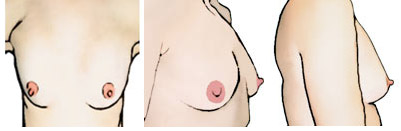
10. Empty or deflated. Commonly after breast feeding. Breast augmentation. See 13 below. (1%)

11. Small breasted. Breast augmentation. (2%)

12. When the nipple is at or below the crease then plastic surgeons consider the breasts to be ptotic (droopy). On side view the nipples are at the crease. Since these breasts are relatively small and only just starting to be ptotic a good result can be achieved with a breast implant which will provide a minor degree of lift. It will, of course, also make the breasts bigger. If you have these breasts, you are happy with their size, but want a small lift then either a Benelli lift or a regular mastopexy could be done. (1%)
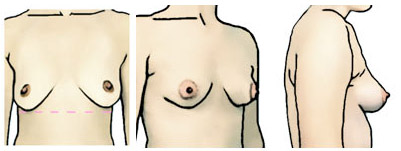
13. Empty breasts, typically after breast feeding. Similar to 18, 20 and 21 below, slightly emptier. What gets done depends on how you feel about size. If you are prepared to go bigger then larger implants and higher profile implants will provide better lift. If you only want to go somewhat bigger then medium size implants may still give you enough lift in the short term, but down the line you may require a mastopexy. Small implants will provide some degree of lift, perhaps not enough and a pexy-augmenation will be required. This is breast implant insertion through a mastopexy (lollipop scar) approach. The implants cannot be too small because implant base diameter should match the diameter of your breasts. (1%)
If you absolutely do not want implants you may have sufficient tissue for just a breast lift and auto-augmentation. Auto-augmentation involves lifting the tissue from the lower breast to the upper. If you have sufficient fat for liposuction then you could also consider doing some autologous fat grafting with the mastopexy.

14. Slightly empty breasts. No significant droop. Breast augmentation to fill out the inner and upper aspect and to improve cleavage. (1%)

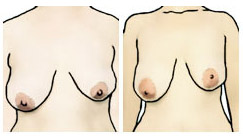
15. Slightly hypoplastic breasts on her frame. The middle and end images show a woman with a slightly fuller figure and she may have enough for autologous fat grafting. For a more predictable result: breast implants. (1%)
16. Slightly hypoplastic breasts on her frame, but with a prominent breast bone and upper chest. Implants are required to improve breast projection and to fill out the lower pole. (0%)
17. Smaller breasts with empty upper poles and poor cleavage. Implants would improve this as well as projection and size. (1%)

18. Similar to 13, 20, 21 but with more droop. The nipples are at the crease, maybe a little below and if this is the case then a breast lift would be required. Implants would provide some lift and may be sufficient for the left pictures. These patients have a range of options and the best one is chosen according to patient desires. (2%)

19. Droopy. The nipples are below the crease and pointing down. Matopexy is required with auto-augmentation (lifting tissue from the lower part to the upper part of the breast). Further volume can be added with either implants (more volume, greater predictability) -mastopexy-augmentation procedure – or fat grafting (less volume, less predictable). (1%)

20. Empty breasts (see 13, 18 and 20), typically after breast feeding. Solutions as for 18. Breast enlargement, mastopexy or both. (0%)

21. Slightly empty, slightly droopy breasts, similar to 13, 18 and 20. Breast enlargement, mastopexy or both. (1%)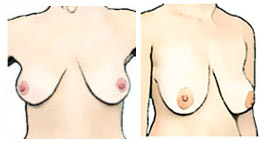
22. Droopy, but with enough volume. Typically I would try to avoid implants in a patient like this and do a conventional breast lift with auto-augmentation. The risk of implants alone in breast like this is a “rock in a sock” appearance. (22%)

23. Droopy. Similar to above. Mastopexy (0%)
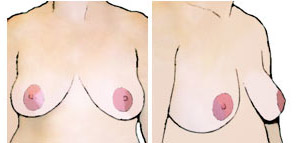
24. These breasts are a little droopy and the patient has a fuller figure. If her body mass index (BMI) is less than 30 then she is suitable for surgery. Mastopexy would be the recommended procedure. A small amount of volume could be added with fat grafting if she is undergoing concurrent liposuction. (2%)

25. Full slightly droopy breasts which would benefit from mastopexy. (0%)

26. Reasonable volume, slightly droopy. Mastopexy. (1%)

27. Empty, flat breasts with some droop. Require a breast lift and possibly some volume. (0%)
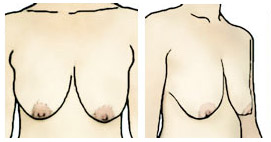
28. Sagging, droopy breasts.Mastopexy. (1%)

29. Patient with a fuller figure and droopy breasts. As long as her body mass index (BMI) is less than 30, she is suitable for surgery. Her breasts are not that larger for her frame and so a breast lift is required, but she would also benefit from some liposuction of the lateral chest wall. (1%)

30. Droopy, a good size, slightly asymmetrical. Mastopexy is the treatment of choice with some tissue removal on the patient’s right side (the left as you view the image). (2%)

31. Large, heavy breasts. Breast reduction (which includes a breast lift). (3%)

32. Overweight patient with empty, droopy and large breasts. She needs to check that her body mass index (BMI) is less than 30. If so then a breast lift/breast reduction would help the shape of her breasts. (2%)

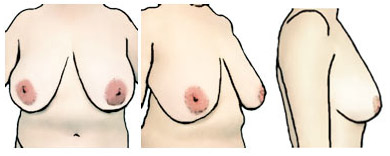
33. Large breasts, full below and relatively empty above. Breast reduction (which includes a breast lift). She has a fuller figure and some liposuction for the lateral chest wall may be beneficial as well. (5%)

34. Large, full breasts. Breast reduction (which includes a breast lift). She has a fuller figure and some liposuction for the lateral chest wall may be beneficial as well. (3%)

35. Large, droopy breasts. Breast reduction (which includes a breast lift). She has a fuller figure and some liposuction for the lateral chest wall may be beneficial as well. Sometimes this upper pole fullness is seen in patients who previously had breast implants put in some years ago and have since put on weight. If this is the case the implants can be removed and the patient usually has enough breast tissue to now go without implants. (1%)

36. Large, droopy breasts. Breast reduction (which includes a breast lift). She has a fuller figure and some liposuction for the lateral chest wall may be beneficial as well. (3%)

37. Large, droopy breasts. Breast reduction (which includes a breast lift). She has a fuller figure and some liposuction for the lateral chest wall may be beneficial as well. (2%)

38. Large, droopy breasts. Breast reduction (which includes a breast lift). She has a fuller figure and some liposuction for the lateral chest wall may be beneficial as well. (2%)

39. Large, droopy breasts. Breast reduction (which includes a breast lift). (3%)
40. Large, droopy breasts. Breast reduction (which includes a breast lift). She has a fuller figure and some liposuction for the lateral chest wall may be beneficial as well. (3%)

41. Large, droopy breasts. Breast reduction (which includes a breast lift). She has a fuller figure and some liposuction for the lateral chest wall may be beneficial as well. (6%)

42. Large, droopy breasts. Breast reduction (which includes a breast lift). She has a fuller figure and some liposuction for the lateral chest wall may be beneficial as well. (6%)

43. Large, droopy breasts. Breast reduction (which includes a breast lift). (5%)
44. Large, droopy breasts. Breast reduction (which includes a breast lift). (6%)

45. Large, droopy breasts. Breast reduction (which includes a breast lift). (6%)

46. Asymmetrical breasts with reasonable volume, but different on either side. The breasts could be lifted with a small reduction on the patient’s right (the left side as you view the image). (1%)
47. Asymmetrical breasts which require a breast reduction (with lift) on the patient’s right (your left as you view the image). The patient’s left breast can be left alone, lifted if necessary, or augmented with implants or fat grafts. (4%)
Thanks for scrolling through. Have you voted? Send me a comment: lazarus@plasticsurgery.co.za
Last updated (with %): 21 August 2019

TESTIMONIALS
6 March 2019
First off – Dr. Lazarus and his team are amazing, they are warm and humble – and you really have a sense of comfort with them. So straight off the bat I can guarantee you are going to be in great hands.
When I went for my consultation, I was obviously a bit nervous, but Dr made me comfortable from the start and went through everything in detail with me, showed me some of his previous patients that did the size I did and showed me that scarring (tiny cut) really heals amazing.
Dani is amazing – I spoke with her straight after Dr Dirk, and she also took me through the whole scenario when surgery happens and where you will be in clinic after surgery. She’s very kind and very sweet.
Anneli is an absolute star – she’s always kind and helpful with anything.
My consultation before surgery – Dani took me through the whole process again, did a medical questionnaire regarding allergies etc, and explains that after surgery she goes through all the necessary details what to do after surgery.
The anesthetist was also amazing – day of surgery she comes in – checks in on you also asks a few questions (medical) and she really comforts you.
Dr Dirk will come in and he will “map” out with a marker pen I assume where he cuts and how he would like for it to “sit” – but that’s quick – I know just before he started drawing on me Sue (the anesthetist) camae and brought me a relaxing pill, because obviously one is always nervous going in for any surgery.
They leave you to wake up on your own in clinic, I went in at 8am and I woke up at 12:30 the afternoon. Surgery is only about an hour.
There’s a nurse that comes in that checks up on you, also very sweet, her and I sat and chatted forever. [That is Elmare]. She brings you something to eat and drink, they want to check that you don’t feel sick, etc.
Once they see you ok, they will release you.
I must admit, from hearing of previous friends that did the same surgery, I was expecting to be in a hell of a lot of pain, but it was all good.
I only struggled in the mornings I think for the first 3 days, the getting up from bed after you have woken up is a slight mission and I know I had a bit of tenderness for about 20min after, but then I would be ok again.
Went for my first post op check up 4 days after surgery and that was super quick, Dr Dirk basically checks in how you feeling, he looks at your bruising and swelling etc and if he sees all is good – you good to go.
He changed my plaster I think Monday that passed now.
The clinic is clean, and as mentioned – Dirk and his team are so helpful, and so kind and they really do email or phone check ins about once a week.
I did my op almost 2 weeks ago, and it was the best experience I’ve had. I’ve had no issues with anything and there were no complications.
In all honesty – this will be the best thing you ever do. And my boobies are still healing 😌”