
Dr. Dirk Lazarus
Plastic, Reconstructive and Aesthetic Surgeon
MBChB (UCT)
FCS (SA) Plast & Recon Surg

Breast Augmentation
If you are uncertain as to which breast procedure(s) might be right for you then have a look at my page on breasts.
Breast augmentation is an operation to increase the size of your breasts with the insertion of breast implants (or occasionally fat, see below). The procedure can also help to improve their shape and symmetry and provide a small degree of lift. The operation is usually done for women with naturally small breasts, or whose breasts have emptied out following pregnancies and breast feeding, and who now want to achieve a greater degree of femininity and better breasts. Going from normal to massive is not something I recommend.
Breast augmentation should only be considered once you have achieved physical maturity and the breasts have ceased to develop further, in general this is after the age of 18. Following pregnancy and breast feeding, breast surgery should only be performed once your breasts have returned their pre-pregnancy/pre-breast feeding state. This usually means at least six months after delivery and at least 3 months after ceasing lactation. Breast augmentation may be used to correct congenital defects of the breast such as tuberous breasts or Poland’s syndrome.
Breast augmentation may done with implants or with autologous (your own) fat grafting. Insertion of breast implants is the usual way of doing breast augmentation as it gives the size increase most women want and is more predictable than using fat. Using your own fat (harvested with a liposuction procedure) requires sufficient fat for the augmentation, costs more (you require the additional liposuction), is less predictable, and really only gives a modest augmentation, less than a cup size. For more on autologous fat grafting see below.
A note on bras and cup size: A breast cup is about 240-250 ml (the same as baking). In fact a cup is half a pint or 8 fluid oz which is 237 ml. The exact same cup would be used for a 32D, a 34C, 36B and a 38A and so band size is important too, but that is not changed with breast augmentation.

A note on pricing. I recognise that for many women price is a barrier to getting breast implants. I also recognise that there are companies and surgeons who offer less expensive breast implant surgery than I do. One way to do breast implant surgery is to make a cut, create a cavity and put some implants in – that is not difficult to do – but there is a certain finesse required in creating breasts which look good and age well. I see a number of patients who have been done where the muscle has been over or under released, where the breast falls off the implant or the implant has been placed incorrectly, where there is bottoming out, long unsightly scars, and shape, size or symmetry issues which could have been avoided or minimised by better surgery initially. The surgery requires care, consideration and attention to detail. I have a philosophy of making each patient the best that I can possibly do and with over 20 years experience doing this surgery and having done all my trial and error learning years ago, I believe that I offer a consistency and degree of satisfaction that is worth it.
There are a number of considerations in breast augmentation. If you are having the surgery please read all the information below.
Below is my Youtube video on conventional breast augmentation with silicone implants. This is an intra-operative video showing surgery, so not for sensitive viewers!
2023 update: minor changes to my surgical technique – how I inject the local anaesthetic, a fourth layer of sutures to fix the scar at the crease and I now use Motiva silk surface implants as opposed to the textured implants shown in the video.
The Surgery
I do all my breast augmentations as day case surgery (in and out the same day) in my own private facility. The procedure is usually done under sedation and local anaesthesia. You will be asleep, pain-free and unaware at the time of surgery – breathing and sleeping on your own – which will allow you to have a quick and comfortable recovery. During surgery an incision is made, then the cavity for the implants. Sizers are inserted into the cavity to test the correct sizing and the shape and size of the pocket. The pocket is then washed out with antiseptic solution, checked again that there is no bleeding and the implants inserted. The cuts are closed with 3 layers of dissolving sutures and no drain. A small dressing is applied and you will be put into a post-opertive support bra which should be worn for 3 weeks. The bra is to help swelling subside and to support the breasts. If the implants are placed under the muscle or in a dual plane position, then I will also put on a band – see the image – to prevent the implants from riding up. The surgery takes about an hour.
Incision
There are a number of options for the incision for breast augmentation.
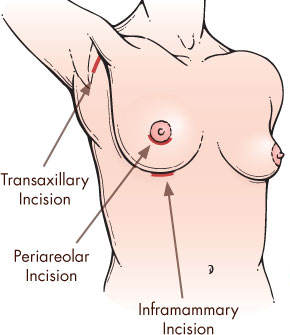
Breast augmentation incision site possibilities.
Infra-mammary crease incision: My default incision is a cut in the crease underneath the breasts. This incision is in natural body tension lines and situated in the shadow underneath the breasts. It is the incision which heals the best and is least conspicuous. Most importantly it allows the most accurate placement of the implants. The incision is usually no longer than 5 cm. For these reasons it is the most commonly used incision.

A mature infra-mammary crease incision.
Peri-areolar incision: Around the areola. I use this in two situations: women who have large areolae and want an areola reduction or in women who may need a small lift. Disadvantages of this approach are that it is some distance away from the cavity and further dissection is required either through or around the breast to place the implant. The scar is left on the breast mound which can be quite visible. The areolae may stretch out and become larger with this incision or a purse-string is used which may be palpable (you can feel it).
An extension of this is the lollipop approach used when I do a breast lift. In addition to a peri-areolar incision a vertical component is needed down to the crease to tighten the skin and to lift the breasts. This is my usual way of doing an augmentation-mastopexy: a breast lift plus implants.
Armpit incision: This goes through a “dirty” area, it is a long way down to the crease to set the correct implant height and a 15% incidence of implant height discrepancy has been reported. The scar in the armpit can be quite visible. Bleeding can be difficult to control. For these reasons, I have abandoned this incision and no longer use it.
Umbilical incision: through the belly button (TUBA – trans-umbilical breast augmentation) is rarely done (7% of plastic surgeons in one survey) and not by me. Special equipment is required, one is confined to saline implants (not as good as silicone) and one creates a cavity from the breast down to the belly button into which the implants can fall. This approach is generally regarded as converting a simple operation into a complicated one and which saves minimal scarring.
Existing scars: if possible, rarely so.
Cavity
Once the incision is done then a cavity is made into which the implants are placed. There are a number of options with the cavity:
Sub-glandular placement: under the breast, but on top of the muscle. This is a quick, easy dissection and I therefore use it when I can which is usually in patients who have a fuller figure. Disadvantages of sub-glandular placement are that the implant may be more visible and palpable especially in the upper and cleavage areas. Visibility can present as a prominent edge, a dome shape to your breasts with a sharp cut-off between breast and chest, wrinkling or folding.
Sub-fascial placement: A thin membrane lies on top of the muscle, the fascia, and some surgeons like to lift this tissue paper thin fascia to allow the implants to sit under the fascia . I do not believe that this adds any benefit to the surgery and so I do not do this.
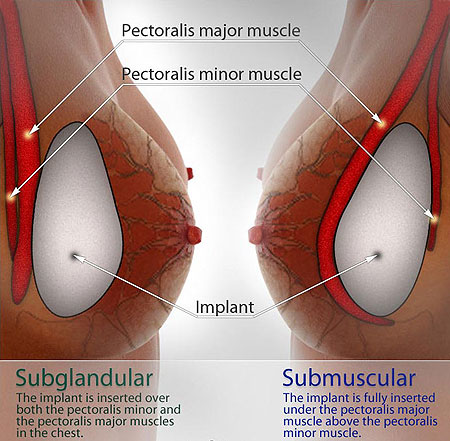
Sub-glandular and sub-muscular placement
Sub-muscular placement: deeper than sub-glandular, underneath the pectoralis major muscle of the chest. Deeper placement, under the muscle, creates more padding over the implant and therefore slightly lowers the risk of capsular contracture and can make the breasts look more natural. The problem with sub-muscular placement, apart from a slightly longer recovery time, is that implant displacement or deformation can occur with muscular activity. I therefore usually perform a dual plane placement.
Dual plane placement: was designed to get the best of both worlds. Lower down and out to the side a sub-glandular pocket is created. This allows accurate definition of the infra-mammary crease (the crease under the breast). Higher up, a sub-muscular pocket is created so that the upper part of the implant and the part along the breast bone comes to lie under the muscle. This creates a more natural look to the upper pole of the breast and cleavage. To minimise implant distortion and displacement, the lower fibres of the muscle are divided to allow the muscle to ride up a little. While recovery is a little longer than sub-glandular placement, the benefits, certainly in thinner patients, make this my default cavity now.
Implants and size
A number of factors need to be considered in relation to the implant itself.
Make: Over the years I have used a number of different makes and although I now offer Motiva and GCA Perlé. These are the latest, generation 6 implants which have a micro-textured (silk) surface to help lower the risk of capsular contracture. The silicone gel inside has also been engineered to be more like the consistency of natural breast tissue.
Shell: All implants have a silicone outer shell which contains the contents. The shell may be smooth, traditionally textured, or micro-textured which I prefer for most patients.
Content or Fill: Traditionally saline of silicone gel. Saline implants can slosh, wrinkle, deflate and are simply bags of salt water which do not have the same feel as breast tissue. Where patients and surgeons have the choice, silicone gel filled implants are by far the most popular choice. Silicone gel fill may have different degrees of cohesivity. Older implants contain non-cohesive silicone – when cut the silicone can leak out and has the consistency of honey. Modern implants have more highly cohesive silicone so that when cut the implant resembles a jelly baby, or, as they are sometimes called, gummy bear implants. The higher the cohesivity, the firmer the implant. I use medium cohesivity implants to minimise the risk of wrinkling and yet keep the benefits of a cohesive implant. See a further discussion on the safety of silicone gel filled implants below.
Shape: Round or anatomical. Anatomical implants have a tear drop shape: fuller in the lower pole and tapering in the upper pole. My preference is for round implants in all breast augmentation patients. Studies show that no one can tell the difference between round and anatomical. Further, anatomical implants rotate and distort the breast. While this may only be clinically apparent in a small number of patients, when patients have an ultrasound scan the vast majority of anatomical implants have rotated to some extent. Finally, anatomical implants are more expensive and firmer. While some surgeons use predominantly anatomical implants, I find it difficult to justify the lack or benefit and potential risks.
Profile: How much the implant projects. Various profiles exist: low, medium, high (full), extra high. For the average patient going from small to a full B or a C cup I usually use a medium profile implant. For women wanting bigger, more projecting breasts – more obviously augmented – a high or extra high profile is used, and while this gives bigger, fuller, more projecting breasts, the bigger one goes the less well your breasts will age.
Percentage fill: All implants that I use are 100% filled.
Size: Most women are most concerned about size. Women are fearful of going too big and looking ridiculous or going too small and being dissatisfied. There are a number of ways of determining size.
- At consultation in-bra sizers will be used so that you can get a feel for the implants of different sizes. This process also makes sure that we are on the same page in relation to sizing and that I understand what you want.
- The bio-dimensional approach is also used. This is based on your breast width and skin thickness. Given a breast of a certain size, and a patient with a certain amount of skin and fat covering, the implant diameter can be calculated so that the implant fills the breast when centred on the nipple-areola.
- Viewing before and after pictures of other patients can be helpful to give me an idea of what you want in terms of size.
- At surgery, once the incision has been made and the cavity created, in-breast sizers are placed to determine what looks right for you, makes you in proportion and is in accordance with your desires in terms of size.

Breast Implants
A few more issues relating to size:
The difference between one size and the next size up or down is 20-25 ml which is only a few teaspoonfuls or about 10% of a cup. It is not a great deal.
Post-operatively you will be swollen, perhaps almost up to one cup size bigger than your final size will be. That swelling will take a couple of weeks to subside.
During that period, in fact, very quickly, your brain will adapt to your new body image.
Over time your breasts will shrink as part of the aging process.
It is therefore possible to wake up from surgery, look down at your breasts and feel that they are too big. Over the next week or two as the swelling subsides and as you get used to the implants, you may feel that they go through a good phase, but end up too small. I am aware of this and my aim is to make you happy in the long term. I will advise you accordingly and ultimately size you to what I believe will give you satisfaction in the long term. If you know what you want then I will get it right and it is very unusual for me to get the sizing wrong – I have done this operation many times before and I like to believe that I understand what most women want when it comes to breast implant size.
Below is my vlog on round vs. anatomical implants – which is better?
Autologous Fat Breast Augmentation: Alternative to silicone gel filled breast implants
If you are small breasted, considering breast enlargement and you have enough fat, you may be suitable for autologous fat breast augmentation (AFBA). With AFBA, the fat is harvested with liposuction and recycled into the breasts. It can give a modest increase in breast size. Sometimes repeat procedures are required to inject more fat to attain the size that you want.
Advantages of AFBA include:
- Minimal scarring: The fat is injected through a 3 mm stab incision in the crease underneath each breast.
- Avoidance of the issues of having an implant. Having an implant can lead to long term issues (see more on this page) including capsular contracture, implant rupture, implant palpability and visibility, folding, wrinkling and the need to replace the implants in due course.
- More natural aging of the breasts. As the breasts age with implants they may start to fall off the implant. With fat grafting the breasts behave in a more natural manner.
- The breasts can be shaped as required – the fat can be placed where it is needed.
- Donor site improvement: the fat is harvested from those fatty bits that most women don’t like: love handles, saddlebags, tummy, thighs, etc.
- The appeal of recycling.
Disadvantages of AFBA include:
- You need enough fat. Of every litre harvested, after treatment only about a third remains for injection.
- Fat take. The fat is injected as a graft, a tissue transfer without a blood supply. For the fat to live in the breasts it has to become vascularized – new blood vessels need to grow in to nourish the fat. This is called “take”. The process of vascularization takes several months and during this period the fat grafts are stressed, and to cope with this, they shrink and some may even not survive. After surgery there will be swelling due to the injection and the trauma of surgery, but this resolves in 2-3 weeks. The breasts may then continue to shrink to close to or even to their pre-surgical state. But as the grafts take, start to thrive and the fat cells again return to their normal size, the results will become more apparent. This should be by 6 months after fat grafting.
- Cancer fears. Initially there were concerns that AFBA might be able to trigger or initiate cancer, but this currently does not appear to be the case. A lot of the initial work on breast fat grafting actually originated (in Italy) on patients who had breast deformities after breast cancer surgery or treatment. In other words, it was breast cancer patients who were receiving fat grafts to the breasts.
- Potential complications: hardness, cysts can occur.
The Surgical Procedure
Surgery is performed as a day case procedure (in and out the same day) in my own, private facility. The surgery is done under sedation and local anaesthesia. You will be asleep, pain-free and unaware at the time of surgery and you will have a quick recovery
Fat harvest is done as conventional liposuction, either with the liposuction machine or with syringe liposculpture (the lipo results do not differ). Usually I start with you lying on your tummy to harvest the fat from the back (love handles, buttocks, thighs, etc) and then we roll you over for harvest from the front (tummy, thighs etc). The harvested fat may be treated with centrifuge prior to injection into the breasts. The fat is transferred to smaller syringes for injection which is done through a small incision under each breast.
After surgery, you will have light dressings as for liposuction. You will be transferred to the ward for discharge later when we are satisfied with your condition. Post-operative care is as for liposuction.
Potential problems or complications which can occur specific to the procedure include the following:
- Hardness
- Irregularity
- Lumps
- Fat cysts
- Inadequate augmentation
- Asymmetry
These complications are rare and the usual outcome from AFBA is satisfactory.
Safety of Silicone gel filled Implants
Most breast implants in current use are made from a silicone shell. This shell may be filled with either silicone gel, saline (salt water) solution or other solutions such as hydrogel, vegetable oils, etc. I still believe that silicone gel filled implants are superior to saline or any other material with regard to look and feel.
Silicone gel implants were first introduced in 1963 and were in wide use up until 1992. In 1992, following a screening of the Connie Chang show on television in the USA, silicone breast implants were placed under moratorium by the Food and Drug Administration (FDA) there. (They were still allowed to be used for breast reconstruction after cancer surgery and they were still allowed to be used in other countries.) The reason for the moratorium was that they were thought to cause human adjuvant disease – a group of arthritis-like conditions which may be associated with rashes, fevers, weight loss, poor appetite, malaise, tiredness and even depression. Silicone breast implants subsequently became the subject of one of the largest class action legal proceedings in history. The company responsible for the silicone, Dow Corning, went insolvent. Other countries followed suit and banned their use.
Since the initial moratorium by the FDA in 1992 much research has been done. This research has been conducted by non-plastic surgeons and physicians with no commercial interest in breast augmentation. In essence it has been absolutely shown that there is no correlation between silicone gel filled breast implants and human adjuvent disease or indeed with any similar condition. Over 20 studies looking at more than half a million women who have had breast implants have found no evidence of breast implants being associated with connective tissue diseases.
The current view of the American College of Rheumatology, the Centre for Disease Control and the American Medical Association is that there is no relationship between silicone breast implants and any disease process and this view has also been formally expressed by the FDA.
The moratorium on silicone gel filled implants was lifted by the FDA in 2006.
Many doctors (not just Plastic Surgeons) feel that the moratorium was too hastily carried out, not well thought through and some have even labelled it hysterical. Silicone gel filled implants still give the most natural look and feel and I still believe them to be the best form of augmentation.
Breast Implant Illness: Systemic Symptoms associated with Breast Implants and Implant removal
Summary: Some women with breast implants may experience a variety of systemic symptoms such as joint pain, muscle aches, confusion, chronic fatigue, autoimmune diseases, and others. Individual patient risk for the development of these symptoms has not been well established. Some patients report complete resolution of symptoms when the implants are removed without replacement. This condition goes by a variety of names including Breast Implant Illness (BII) and Systemic Symptoms associated with Breast Implant (SSBI).
What we know:
- Systemic symptoms patients attribute to their breast implants have been reported with all types of implants: saline and gel filled, smooth and textured surfaces, and has been reported with implants from every manufacturer.
- Over 100 symptoms have been reported, in no specific configuration.
- Some patients will experience symptom improvement with implant removal.
Patients should know:
- Breast implants are not lifetime devices and require regular follow-up.
- Implant integrity should be evaluated with high-resolution ultrasound (HRUS) or MRI five years after implant placement and every 2–3 years after.
- Any persistent symptoms that occur in patients with breast implants should be evaluated for other medical diseases prior to consideration of undergoing implant removal surgery.
- For patients who develop symptoms that they attribute to their breast implants, if no other cause is found, it is likely that they will see at least partial symptom improvement after implant removal. The symptom improvement may occur with no or partial capsulectomy which is a procedure that is less invasive, less expensive and may carry lower risk.
- Patients should seek certified plastic surgeons for any concerns with their breast implants.
Safety Advisory from ISAPS here
PIP Implants
Poly Implant Prothèse (PIP) was a French company founded in 1991 that produced silicone gel breast implants. The company was preemptively liquidated in 2010 after it was discovered that they were using inferior grade silicone in their breast implants.
The CEO of the company, Jean-Claude Mas, is currently serving a prison term. Despite the fact that his factory was regularly inspected and that PIP implants were certified and CE mark approved, he still managed to deliberately hide from the regulatory authorities that he was using an inferior grade of silicone.
PIP was the 3rd largest maker of breast implants. The company sold about 2 million sets of implants in its 20 year history. About 300 000 women are estimated to have received PIP implants in 65 countries, including Britain (47 000 women), France (30 000 women), Germany, Italy, Spain, many countries in South America, Australia and South Africa. In South Africa it is unknown how many women received PIP implants, probably several thousand. Unfortunately I was one of the surgeons who used PIP implants, although by 2005 I had moved mostly to other brands.
What is the risk with these implants?
The risk is that these implants have a higher rupture rate. Rupture is when the shell of the implant breaks and the silicone gel from the inside can leak out. The rupture rate with PIP implants is thought to be about 2 to 5 times higher than normal. The French health authorities, Agence française de sécurité sanitaire des produits de santé (AFSSAPS) monitored and registered 672 preventive extractions – removal of PIP implants – and in 43 cases (6.4%) the implants had ruptured. A study in the Journal of Plastic and Aesthetic Surgery revealed that, in an audit of 453 patients who had PIP implants, between 16% and 34% of the implants ruptured. This compared to a failure rate of less than 1% in other implants. The UK Department of Health states that despite the use of non-medical grade silicone in PIP implants, there are no lasting health risks if they do rupture.
What are the signs of implant rupture?
Implant rupture is usually silent. In other words, you would not know. Leaking silicone is unlikely to have systemic (general) effects – none have been proven – but the free silicone can have local effects, mainly something called siliconomas. These present as lumps of tissue around the free silicone. Sometimes it can present as soreness, redness, lumpiness and pain in their breast or as an enlarged lymph node (lump) in the armpit which may be tender. Implant rupture can be detected on an ultrasound scan of the breast, mammogram or MRI scan (magnetic resonance imaging).
Can PIP implants or ruptured PIP implants cause cancer?
An independent expert committee, led by NHS medical director Professor Sir Bruce Keogh, found the materials used in PIP implants are neither toxic nor carcinogenic. The European Commission’s Scientific Committee on Emerging and Newly Identified Health Risks (SCENIHR) October 2013 report confirms this and adds that “there is no reliable evidence that ruptured PIP implants create a greater health risk than a ruptured silicone breast implant from another manufacturer”.
Do PIP implant need to be removed?
Some countries, including Sweden, Germany and France, have urged women with PIP implants to have them taken out as a safety measure. In the UK, official government advice is that there is no need to have the implants removed unless they have ruptured, or if you feel anxious about leaving them in. Here in South Africa, our Association has recommended the following: “In the absence of clinical symptoms of rupture, patients should not be advised to seek explantation, but should have regular follow up examinations and yearly sonar appraisals.”
What does implant removal/exchange entail?
If you feel anxious about having PIP implants in you and you want to change your implants or if you are considering further breast surgery, then removal can be done. The surgery is done in a manner similar to your prior breast augmentation procedure. The old scars are usually used, so no new scar is created. The implant is removed and the cavity cleaned out. Generally I will recommend a pocket change from sub-glandular to the more modern dual plane pocket which places the upper part of the implant under the muscle. In most cases it is recommended to insert a new implant rather than not to. Leaving out the implant will leave loose skin (it has been expanded by the implant) and empty breasts. The skin would need tightening which would require additional breast cuts.
What are the costs involved in implant exchange?
Here is the statement from our Association: “This then raises the unpleasant topic of financial obligations. Clearly at the time of implantation the surgeon had no reason to believe that he/she might be inserting faulty devices and as such, cannot be financially penalized for the Company’s dishonesty and indiscretion. Due to the sensitive nature of the problem and in light of preserving our stature in the Health care environment, we will try to help these patients to effect necessary changes. It should be explained that we have the patients best interests at heart and are doing everything in our power to help resolve the problem.”
All patients who have received PIP implants from me can see me anytime for consultation at no cost.
The cost of scans is determined by the radiologists who perform the scans.
The chief Medical Officer in the UK, Dame Sally Davies says: “Women with PIP implants should not be unduly worried. We have no evidence of a link to cancer or an increased risk of rupture [not sure she right about that]. If women are concerned they should speak to their surgeon.”. Removing the implant “carries risks in itself,” she also said.
Post-operative
Following surgery you will be transferred to the ward. You can be discharged later in the afternoon once we are satisfied with your condition.
Post-operatively you can expect some pain for which we will give you pain killers to take home. Pain thresholds vary from patient to patient – some women are fine after 3 days, others need a week. When you can lift and move your arms easily, then driving can be resumed, usually by about a week after surgery. A few days to a week off work is usually all that is required. Gym and exercise can be resumed after about 3 weeks.
Bruising will last about 10 days to 2 weeks, swelling a little longer. These are the usual durations which may vary. Final appearance is only achieved months after surgery. For all surgery, an exact end-result cannot be predicted due to uncontrollable factors such as how you scar, etc.
The first check up will be within a few days of surgery and regular follow ups will be done after that. If you experience any problems it is better to contact me. I prefer to find out that it is nothing serious early rather than to wait to discover a problem. I suggest a 12-14 day duration of stay for patients who are not from Cape Town. You should remain in Cape Town for this period.
Complications
All surgery carries the potential for risks and the possibility of complications. Risks, however are low and complications are rare. Minor complications are more common than major complications. If a complication occurs then my policy is to aggressively manage it. This may not need surgery, but certainly I will want to see you more frequently to ensure that your recovery goes as smoothly as possible.
Anaesthetic related problems: All surgery and anaesthesia carry a risk. That risk is probably equivalent to the risk of flying.
Bleeding: The risk of bleeding is low, around 1-2%. Bleeding into the breast, if it occurs, typically does so early after surgery. The symptoms of a bleed are increased pain associated with marked swelling and possibly more bruising on the side of the bleed. Treatment usually requires a return to theatre to drain the haematoma, stop the bleeding. The cost for this additional surgery is not included in my initial quote for surgery. Bleeding may carry a slightly increased risk of capsular contracture (hardness – see below) down the line.
Infection: Infection may be minor or major. Minor infection – a bit of redness, pain and perhaps a low grade fever – can be managed with antibiotics, perhaps over a longer than normal course. Severe infection can manifest as a wound breakdown with pus and exposure of the implant. This usually requires the implants to be removed to allow the breasts to settle down. The implants can be replaced after 6 months.
Wound healing problems: either impairment or delay. Slow or deficient wound healing (made worse by smoking) can result in skin or tissue loss and require dressings for a prolonged period of time to allow healing.
Nipple-areola loss: Due to interruption of the blood supply to the nipple areola can occur with any breast operation, but is very rare after breast augmentation.
Numbness: The nerves to the breast are microscopic and can be injured (cut, bruised, pulled, etc) during the process of cavity creation. Most patients will experience some degree of numbness following surgery, usually a patch on the lower part of the breast which slowly resolves (over months) and usually returns to normal. Loss of nipple areola sensation, even erogenous sensation can occur, but this is rare.
Scars: How well you scar is largely a function of your skin type. I will suture you up as best I can, but some people do form bad scars. In the early part of the healing process, the scars may be red and raised, but after a few weeks this will settle down. To minimise the scarring response in the wound you should tape the wound with micropore tape. The tape should be applied and then left in position along the scar until it starts to peel off – usually after a week or ten days. The tape should then be removed and re-applied. For optimal scars you should continue this until the scar is no longer red or raised – usually a period of 6-12 months.
Cosmetic problems: This primarily relates to problems of size, shape or symmetry.
- Size: too big or too small. As mentioned above, this is rarely a problem. The larger your implant, the worse your breast will look over time. A larger implant will stretch your tissues over time and will cause more tissue-thinning and sagging than a smaller implant. Your tissues do not improve with age, and they will be less able to support the additional weight of any implant, especially a larger implant.
- Shape: Abnormalities of shape are possible, but rare. Perhaps the most common is a “snoopy droop” appearance when the breast hangs off the implant.
- Symmetry: No woman has truly symmetrical breasts, but what one wants to achieve is acceptable asymmetry. Pre-existing asymmetries in breast size tend to be made less by increasing the breast size and in markedly asymmetrical cases I will use different sized implants. Asymmetries can also occur due to differences in implant position. Most asymmetries are due to pre-existing differences in nipple or crease height or in breast size.
Implant related complications: These include:
- Wrinkling: usually seen along the inner or outer edge of the implant.
- Folding: A folded implant can present as a pointy breast lump. Sometimes this is intermittent or goes on its own or can be manipulated away.
- Palpability: The ability to feel the implant. If you can feel your ribs with your finger, beneath the breast or at the side of your breast, you will be able to feel the edge of your implant beneath your breast and at the side of your breast. Currently manufactured implants that strive to achieve durability of the shell have a thicker shell to prolong the life of your implant, and a thicker shell may be easier for you to feel. If feeling an edge of an implant shell could be a problem for you, do not have an augmentation. We cannot change the quality or thickness of your tissues. If you are thin or have very little breast tissue, you will be more likely to feel your implant. Any implant will feel firmer than a normal breast, regardless of the filler material. If the implant shell folds, it could fail sooner and require you to have a re-operation sooner (most patients accept a firmer breast in exchange for a possibly longer life of the implant shell).
Emotional changes: Prior to surgery you are healthy, but surgery induces the sick state – you will be sore, bruised, swollen and tender. You will need downtime and not be able to do the usual things you do for a few days. These changes can affect some patient’s moods and you may find that you become tearful or depressed for a few days post-operatively.
Long-term Issues and Complications:
1. Capsular Contracture
Around every breast implant, the body will form a capsule composed of fibrous and cellular material. In most women, this capsule remains soft and pliable and does not cause problems. However, in a small percentage of women, the capsule can become firmer and harder resulting in discomfort or even pain, distortion and hardness. This is called capsular contracture.
With modern implants, rates of formation of capsular contracture are relatively low, probably around under 1% per year and some studies show the rate at 10 years to be about 2-3%. However the risk increases the longer the implants have been in. The treatment for developed capsular contracture is surgery: removal of all or part of the capsule (capsulectomy) and replacement (modernisation/upgrade) of the implants. This operation can be combined with breast lift or other surgery which may be required or desired at that time.
2. Leak or Rupture
Leak or rupture of the implants can occur due to trauma such as a motor vehicle accident or due to wear and tear. Modern implants have a very low rupture rate and with cohesive silicone gel as a filler, the silicone does not leak out as happened with older implants. If modern, cohesive gel implants are cut, the surface is like a jelly baby (so called gummy bear implants). Leak or rupture can be diagnosed on a scan of the breast (MRI and ultrasound) and since recommended screening for breast cancer involves mammograms and ultrasound of the breast, leaks may be detected on routine scanning. If you are involved in some traumatic event and are concerned about your implant, then a scan can be arranged. Ruptured implants can result in silicone leak. It is now well proven, by non-plastic surgeons, that silicone gel has no effect on your body and the silicone controversy has been proven to have no validity at all. Free silicone in the breast, however, if left, can result in the formation of lumps called granulomas or siliconamas which require surgical removal. Otherwise a ruptured or leaking implant should be changed which would require surgery.
3. Fertility
Breast implants have no effect on your fertility or ability to fall pregnant.
4. Breast Feeding
Breast implants are placed either under the breast or under the muscle and so do not interfere with your ability to breast feed.
5. Cancer and lymphoma
Breast implants do not cause cancer. In fact in large studies where age and risk factor matched groups of women are compared, one set with implants, the other without, the rate of breast cancer occurrence is slightly lower in those women who have had breast implants. The reason for this is unknown, although it might be due to the fact that these women have smaller breasts and therefore less tissue to become cancerous.
ALCL: also called BIA-ALCL – Breast Implant Associated Anaplastic Large Cell Lymphoma – has been described in a very small number of patients who have had breast implants. In January 2011, the United States Food and Drug Administration (FDA) published an investigation of ALCL and breast implants, which concluded that there is a possible association between breast implants and ALCL. However, only a few published cases have been reported worldwide. Approximately 10 million women have received breast implants . Currently there only about 200 cases of ALCL reported. It is very rare.
ALCL occurs in the capsule around the breast implants. It is a cancer of the immune system, not a cancer of the breast. It presents as changes in the breast: swelling, lump, asymmetry or pain, typically years after receiving implants. In most women, implant and capsule removal have been curative. It seems to be associated more with one make of implants, a make that I do not routinely use. For more information, see the FDA video here, FDA information here (same as the video), and the advice of the British Association of Plastic, Reconstructive and Aesthetic Surgeons (BAPRAS) here. The American Society of Plastic Surgeons also have very good information on their site which you can find here.
6. Cancer screening
Cancer screening can proceed as normal by monthly self examination and regular mammography and ultrasound after the age of 40 or as recommended. Note that for mammography special views will be required to see around the implant and that with sub-glandular implant placement there is the theoretical risk that some breast cells will be left below the implant and that these may not be visualised by routine breast cancer screening techniques.
If you want a totally natural breast, you should not have a breast augmentation.
Young women should take into account that they may well need to have their implants changed or further breast surgery at some point later in life.
For all surgery
Please note the following points:
The practice of medicine and surgery is not an exact science. You should therefore understand that no guarantee or assurance can be given as to the results that may be obtained. Even reputable practitioners cannot guarantee results.
The two sides of the human body are not the same and can never be made the same.
Complications are rare and complications requiring revision surgery even more rare. If complications occur, then this is usually soon after surgery. Complications will be dealt with as appropriate and generally aggressively managed, but most complications will end up healing and improving as time goes by.
More on Complications of Breast Augmentation (from the British Association of Aesthetic Plastic Surgery: https://www.baaps.org.uk/patients/procedures/1/breast_augmentation).
Complications associated with the surgery
- Scars There will be scars from the surgery. These will usually be red at first, then purple, and then fade to become paler over 12 to 18 months. Occasionally, scars may become wider, thicker, red or painful and you may need to have surgery to correct them.
- Bleeding Bleeding around the implant (haematoma) is unusual but possible, and you may need another operation to stop the bleeding. Bleeding usually happens immediately after, or soon after, surgery. Before the surgery your surgeon will discuss any medicines that increase your risk of bleeding, and it is important to control high blood pressure.
- Seroma This is where fluid collects within the breast cavity. It may need to be drained by having a needle through the skin, or by having another operation, and can affect the final result.
- Infection If you get an infection of the wound or around the implant you may need antibiotics or another operation to remove the implant. It is normal to wait at least three to six months for the infection to clear before a new implant is inserted.
- Extrusion This is where deep stitches poke out through the skin. These can easily be removed.
- Swelling, bruising and pain There will be some swelling and bruising of the breasts after the operation, and this can take weeks to settle. There may be long-term pain, but this is uncommon.
- Asymmetry This is where the breasts are not symmetrical.
- Increased or reduced sensation After the surgery, most patients will get some alteration in the sensation in their breasts, most commonly numbness near the scar and oversensitivity of the nipples. Loss of sensation to the nipple, though rare, may be permanent. Rarely, the loss of or increase in sensation can affect breastfeeding.
- Damage to deeper structures Although rare, the surgery can damage deeper structures, including nerves, blood vessels, muscles and lungs. This damage may be temporary or permanent.
- Unsatisfactory result Sometimes, patients are not satisfied with the result of their breast augmentation surgery. This may be to do with the look or feel of the breasts, or the breast shape not meeting expectations. It is very important that you talk to your surgeon, before you have the surgery, about the size and shape you want, and whether this can be safely achieved with a good outcome.
- Change over time The appearance of the breast will change as a result of aging, pregnancy or other circumstances not related to your surgery, such as putting on or losing weight. You may need further surgery or other treatments to maintain the results of the breast augmentation. Many patients choose breast augmentation because they feel the skin on the breast is loose or saggy, and they want the implant to fill the skin out. You should bear in mind that large implants are heavier and the weight of them can make the breast droopy in the future, and so you may need a further operation. Sometimes, having a breast uplift would be preferable to using an overly large implant.
- Allergic reaction Rarely, local allergies to tape, stitches or solutions have been reported. If you have an allergic reaction you may need extra treatment.
Complications associated with the implant
- Capsular contracture It is normal for a scar or capsule to form around the implant. This usually feels soft and looks natural. In about 10% of patients, the scar contracts around the implant and feels firm. If this happens, the breasts can feel tender and look abnormal, and you may need an operation to replace the implant. After 10 years, about 10 to 30% of women will have had another operation, and painful or unsightly capsular contracture is the most common reason for this.
- Noticable implants Slim patients may be able to see or feel the edges of the implant. With time, ripples or folds may be noticeable. Very occasionally, teardrop implants can rotate behind the breast. These can usually be pushed back into position gently, but if the problem is persistent, an operation may be needed.
- Implant failure Occasionally implants can leak. This can be as a result of their age, an injury or a tight capsule. Normally the leak is contained within the capsule and does not cause a problem. If the size, shape or consistency of the breast changes as a result, a further operation may be needed to replace the implant.
- Breast droopThe breast may droop over time due to the weight of the implant
Risks of anaesthetic
- Allergic reactions You could have an allergic reaction to the anaesthetic.
- Chest infection There is a small risk of chest infection. The risk is higher if you smoke.
- Blood clots Blood clots can form in the leg (called a deep vein thrombosis or ‘DVT’). These cause pain and swelling and need to be treated with blood-thinning medication. In rare cases, part of the clot breaks off and goes to the lungs (called a pulmonary embolus or ‘PE’). The risk of this is higher if you smoke, are overweight or are taking the contraceptive pill.
- Heart attack or stroke A heart attack or stroke could be caused by the strain surgery places on the heart. You will be assessed for the risk of this before your surgery.
- Death As with all surgery, it is possible to die as a result of the operation.
Exercise after Breast Implant Surgery
Patients should start light walking immediately after surgery – nothing strenuous, just short walks around the room or home every other hour. This is good for the circulation and helps prevent blood clots. After two weeks, patients can start more intense cardio such as walking on a treadmill or walking uphill. At a month most patients can resume most exercise except heavy lifting. At six weeks, patients are generally completely healed and can resume all exercises.
After breast augmentation, especially with implants under the muscle, I recommend patients try to avoid strenuous chest exercise such as push ups. Since the implants sit under the muscle, contraction places downward and outward pressure on them which, over time can result in the implants dropping or becoming displaced over time. As a general rule, I also tell patients to listen to their bodies – if they do something that causes swelling or discomfort, stop doing it and give it a little more time.
Implants shouldn’t impede you from having an active lifestyle. It is recommended that you use a good supportive bra when exercising.
Longevity of Breast Implants
How long will your implants last? Unfortunately there is no fixed answer to this and it is impossible to say how long your implants will last. Implants may ‘fail’ at any time after surgery. Failure may be due to leakage, significant capsular contracture, wrinkling or other causes. The risk of these events is small early on but increases with time. I advise patients, especially young patients, that they will need to have their implants changed in time. The Allergan and Mentor studies show that about 1 in 5 women will have secondary surgery by 10 years, but that is not to say that the implants will last 10 years or need to be changed at 10 years.
For many women, the result of breast augmentation can be satisfying, even exhilarating, as they learn to appreciate their new, fuller appearance. Your decision to have breast augmentation is a highly personal one that not everyone will understand. The important thing is how you feel about it. Overall, despite much of the previous media hype around breast augmentation, it is one of the better procedures offered by plastic surgeons and one with a high degree of patient satisfaction.
Updated 13 June 2026

May 2023
Dear Dr L,
I hope this note finds you well. I wanted to take a moment to express my heartfelt gratitude for the incredible job you did with my recent surgery. I cannot thank you enough for your expert care and attention to detail throughout the entire process. From our initial consultation to the follow-up appointments, you and your team were attentive, compassionate, and professional, which put me at ease.
Your expertise is truly remarkable. I am beyond grateful for the positive changes you made to my appearance, which has significantly boosted my confidence. The care and concern you showed for my well-being before and after the procedure were exceptional, and I feel incredibly blessed to have had you as my surgeon.
I am well aware that it takes a great deal of skill, dedication, and passion to do what you do. I want you to know that I deeply appreciate your hard work and expertise. You have not only changed my physical appearance but also my life, and for that, I am forever grateful.
Once again, thank you for your exceptional care and expertise. I have nothing but the highest praise for you and your team. You have given me a renewed sense of self-confidence and hope, and I will always remember the amazing work you have done.
You’re my hero ❤️
Incredible Doctor
Thank you again Dr Lazarus
21 March 2019
27 Nov 2018
I’m a week post op and things are good, just had dressings removed today and scars healing well. Dr Lazarus and his team were amazing, made me feel comfortable. He listened during my initial consultation and understood what I was going for. Having lost a lot of weight over the last year, I was not feeling like myself. Breast augmentation was not something I’d ever considered before, and even now I was happy enough – it wasn’t causing self-esteem issues or anything. I just thought it would be a nice extra bonus. Didn’t want anything dramatic.
Healing has gone well, was off painkillers by day 3, almost no bruising, they’re already softer and more natural looking than day 1.
All in all, I think the key for me was understanding what I wanted, having a skilled and empathetic doctor who listened and who I could trust, and also having reasonable expectations myself. I didn’t want to look entirely different, or have something that didn’t fit my body. I did loads of research on what to expect and I feel I’m just allowing the process to happen and not stressing over daily little changes.
I ended up needing 275cc in one side (our original plan) and 300cc in the other, to even things out. Happy with the results!
4 Aug 2016
29 Oct 2017
…I am very happy with how my incisions have healed so far and I am also very pleased with the placement of the scars (it can’t be seen when I’m in a bikini and I have to lift my breast to see the scars when looking in a mirror)…. I’d also like to add that I am extremely happy with the results of my surgery and that my breasts are soft, natural looking and are the perfect size for my frame.
1 Mar 2017
BEST EXPERIENCE- 27 yrs, Female, CT Local, 7 star treatment
Being a little nervous for my procedure prior to surgery, I resulted in feeling very safe in the hands of Dr Lazarus and his team, who are by far the most attentive medical practitioners that I have ever experienced. From the moment you walk into his practice, you feel as though you are at home. From my consultation period, right through to the follow up consultations post surgery, the Tranquility Clinic team have been incredible- always available for any questions and extremely patient and compassionate. I highly recommend Dr Lazarus and couldn’t thank him enough for the incredible artwork that he has created for me.
JasmineTestimonials

Jade Fairbrother, above, South Africa’s first playmate of the year, writing to me and a prospective patient for breast augmentation:
I am one of your biggest advocates, as you know, but of course going through any type of cosmetic or corrective surgery would be daunting the first time or maybe even the second so I can understand how it would be nice and possibly comforting having a secondary opinion from someone who has been through it before – someone who can relate.
L*****, should you decide to go ahead with your procedure I know you won’t regret it – it is life changing and if anything you will wonder why you waited so long before going through with it. Also I can assure that you are not only in the safest but one of the best hands in South Africa, models fly in from across the world and have their augmentations done with Dirk.
Dr. Dirk has also done other procedures for me such as using my own fat as filler to help correct my eye troughs (tired eyes) and fill out my almost none existent top lip. He really is the best of the best!
